|
|||
| LEAD Action News vol 11 Number
3, June 2011, ISSN 1324-6011 Incorporating Lead Aware Times (ISSN 1440-4966) & Lead Advisory Service News (ISSN 1440-0561) The journal of The LEAD (Lead Education and Abatement Design) Group Inc. Editor: Anne Roberts |
|||
|
About Us
|
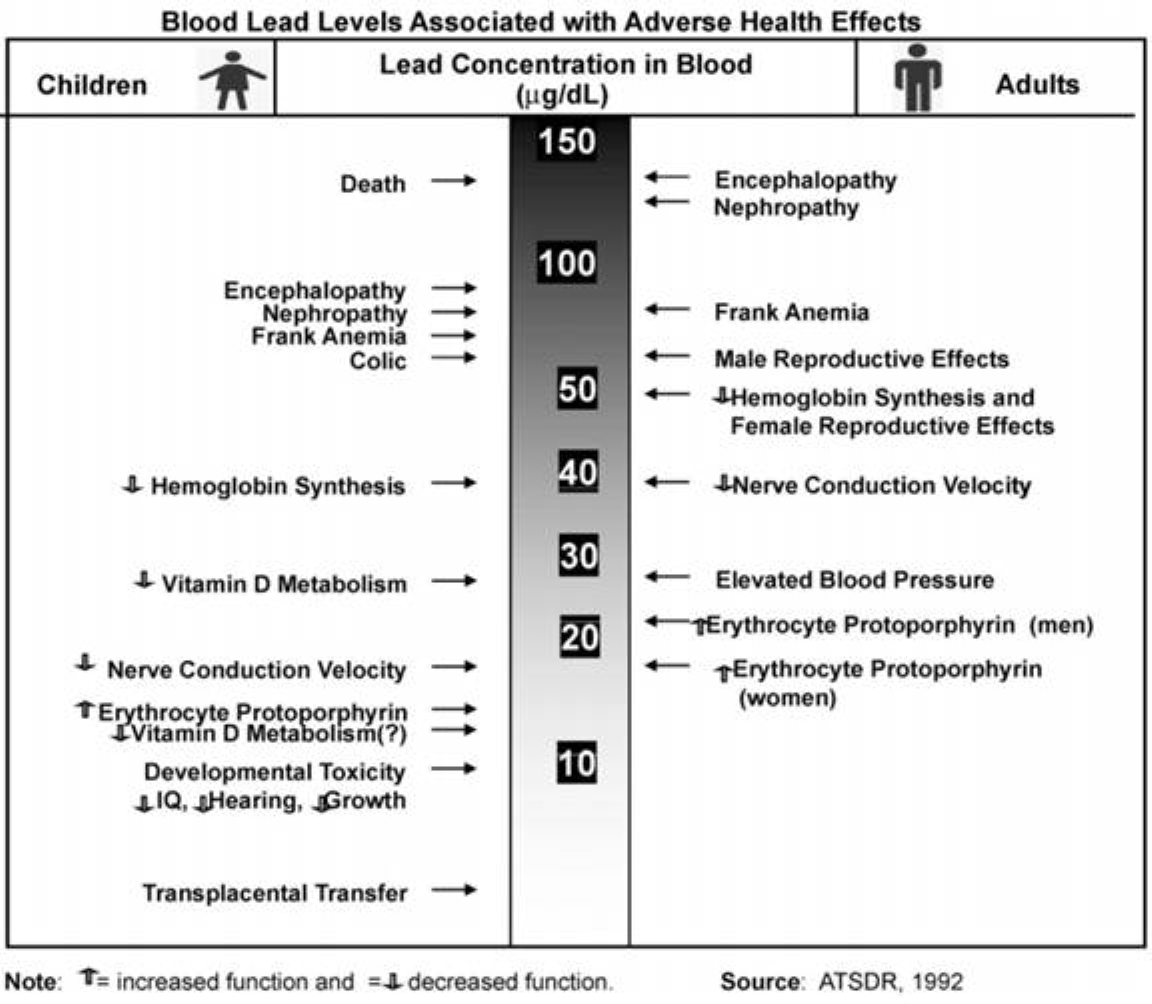
Lead poisoning in China By Russell Ng and Hannah Beedham, Interns from Macquarie University Part III - Treatment and prevention of lead poisoning Part I - Background: Sources of exposure to lead. How does lead enter the body? How does lead affect the body? What is the safe limit for blood lead levels? Sources of exposure to lead Lead is an abundant heavy metal with many practical uses in the production of industrial products such as batteries, metal products such as solder and pipes, ammunition, and devices to shield X-rays (ATSDR 2007). Lead had also found its way into the daily life of people by means of house paints, smoking, printing materials, electronic products, toys and stationery, just to name a few (Dai and Fan 2007). However, amidst the flurry of health concerns surrounding the lead exposure of children which interfered with their psychological and physical development in the mid 20th century, action was taken by many Western countries to ban or greatly reduce lead exposure to the public. This included banning leaded as well as lead-based paints (Crow 2007) ; the former was accomplished at a national level in China by 2002, but the same level of success cannot be said about lead- based paints produced in the factories of China, as a study showed that the lead content was very high in existing painted houses and in new paint available for housing (Lin et al. 2009). However, lead-based paints are only one of the many sources of lead exposure to the Chinese public - in fact, the scope of lead pollution has expanded through electronic products and waste materials released into the atmosphere, water supply, and soil – all by-products of the spread and development of industry in the rural and township areas (Dai and Fan 2007). How does lead enter the body? Lead can enter the body in two ways: inhalation and ingestion. Inhalation of lead dust is a common way for lead to get into the body. When lead is inhaled, about 30-50% of the lead particles will reach the lungs, depending on the size of the particles. Large particles land in the upper respiratory tract, and unfortunately get trapped in mucous and then are often swallowed, allowing the particles to enter the digestive system. The smaller particles can reach deeper into the lungs, where they can be absorbed into the bloodstream (LWD 1998). Lead can also be ingested through foods we eat, from hand-to-mouth activity from lead in dust and soil, and from drinking water, if it has flowed through lead pipes/fittings. It is through ingestion that a higher proportion of lead spreads to other parts of the body via the blood stream (EPA c.2002). From the digestive system, adults will absorb 10-15% of the lead, while children and pregnant women can absorb up to 50% of the lead into the bloodstream. Furthermore, people who are fasting, or if their diet is lacking in iron or calcium, will absorb more lead (LWD 1998). How does lead affect the body? Lead is of no benefit to the body at all, and remains in the body for varying periods of time, depending where in the body it is. Half the total amount of lead in the blood will be excreted in 25 days, or 40 days if in soft tissue, and as long as a few decades in teeth and bones. As a result, a person will continue to be exposed to lead internally even after the exposure to lead stops, and any other bout of exposure will cause lead to continue to accumulate in the body. The total amount of lead that is stored in the body is called the “body burden” and in adults the bone and teeth contain about 95% of the body burden. Lead stored in bones can sometimes leave them and enter the blood and move into soft tissue i.e., the organs, causing damage to them (LWD 1998). Lead affects virtually every system in the body; such as the reproductive, neurological, haematopoietic (pertaining to the formation of blood or blood cells) hepatic, and renal systems (Al-Saleh et al 2009). The adverse health effects of lead and associated blood lead levels can be summed up by the following figure:
Note on some definitions of the health effects: An increase in erythrocyte protoporphyrin is an increase of a certain compound (zinc protoporphyrin) found in red blood cells when heme (a component of hemoglobin, which transports oxygen around the body) production is inhibited by lead and/or lack of iron (Labbe et al 1999). Colic refers to abdominal pains. Frank anemia is associated with unusually smaller and paler than normal of red blood cells. Nephropathy refers to damage to the kidney. Encephalopathy refers to a syndrome of global brain dysfunction. Children are more susceptible than adults to the effects of lead exposure, as a larger proportion of lead ingested is absorbed: more circulating lead enters the brain, and their developing nervous system is more vulnerable to the toxic effects of lead (Meyer at al. 2008). What is the safe limit for blood lead levels? The World Health Organisation’s "safe" limit for lead in blood, originally set in 1995, is 10 µg/dL (micrograms per deciLitre); that is, 100µg/L. (Many sources will interchange between deciLitre and litre for their measurement of blood lead levels). However, even with this "safe" limit put in place by the WHO, there is no detectable safe blood lead level, as at every measurable level of lead there is associated harm (Lee and Chen 2008). Repeated studies have shown that blood lead concentrations at 5 µg/dL impact normal brain development in children as well as being associated with hypertension, heart disease and strokes in adults (OKI 2009). In fact, numerous studies which observed children aged between 6 and 16 have found that there was an inverse relationship with blood lead levels and cognitive development, even when the blood lead levels were less than the “safe” blood lead level of 10µg/dL. A similar study followed a cohort of children and tested them at ages 12 and 24 months and found a significant inverse relationship between blood lead level and mental and psychomotor development, even though their blood lead levels never exceeded 10µg/dL. These findings are important, in that they have identified that there is no threshold for cognitive impairment due to lead exposure in children (Meyer et al 2008). Other standards for lead exposure: In 1971, China's occupational exposure limits (OELs) were based on maximum allowable concentrations at 0.05 mg/m3 for lead dust and 0.03 mg/m3 for lead fumes. However, results from a comprehensive industrial hygiene survey conducted by the Chinese Ministry of Health in 1971-1981 found that the average exposure levels were 2.22 mg/m3 for lead dust and 0.68 mg/m3 for lead fumes. This lead to the passage of the Occupational Diseases Prevention and Control Act in 2002, where new regulatory standards were based on time-weighted averages (TWAs) and short-term exposure limits (STELs). The TWAs are 0.05 mg/m3 and 0.03 mg/m3 lead dust and fumes respectively, and corresponding STELs are 0.15 mg/m3 and 0.09 mg/m3 for lead dust and fumes, respectively (Ye and Wong 2006). However, the 2002 Act appears to have a minimal impact. Lead poisoning rates among lead battery workers dropped from 45% in 1990-2002 to 36.8% between 2003 and 2005. Go and Scull (2008) pointed out that a lead poisoning rate of more than 30% is hardly acceptable. In 1986, the Joint FAO/WHO Expert Committee on Food Additives (JECFA) established a provisional tolerable weekly intake (PTWI) of 25 µg of lead per kg of body weight for infants and children, which was extended to all age groups in 1993. The PTWI was based on metabolic studies in infants which showed that a mean daily intake of 3-4 µg/kg of bodyweight was not associated with an increase in blood lead levels or in the body burden of lead, whereas 5µg/kg of body weight or more resulted in lead retention (WHO 2009). |
||
|
About
Us |
bell
system lead poisoning |
Contact Us
| Council
LEAD Project | egroups | Library
- Fact Sheets | Home
Page | Media Releases Newsletters | Q & A | Referral lists | Reports | Site Map | Slide Shows - Films | Subscription | Useful Links | Search this Site |
|||
| Privacy Policy | Disclaimer | |||
|
Last
Updated 25 January 2012
|
|||